
Why Aren't We Testing For Hantavirus?
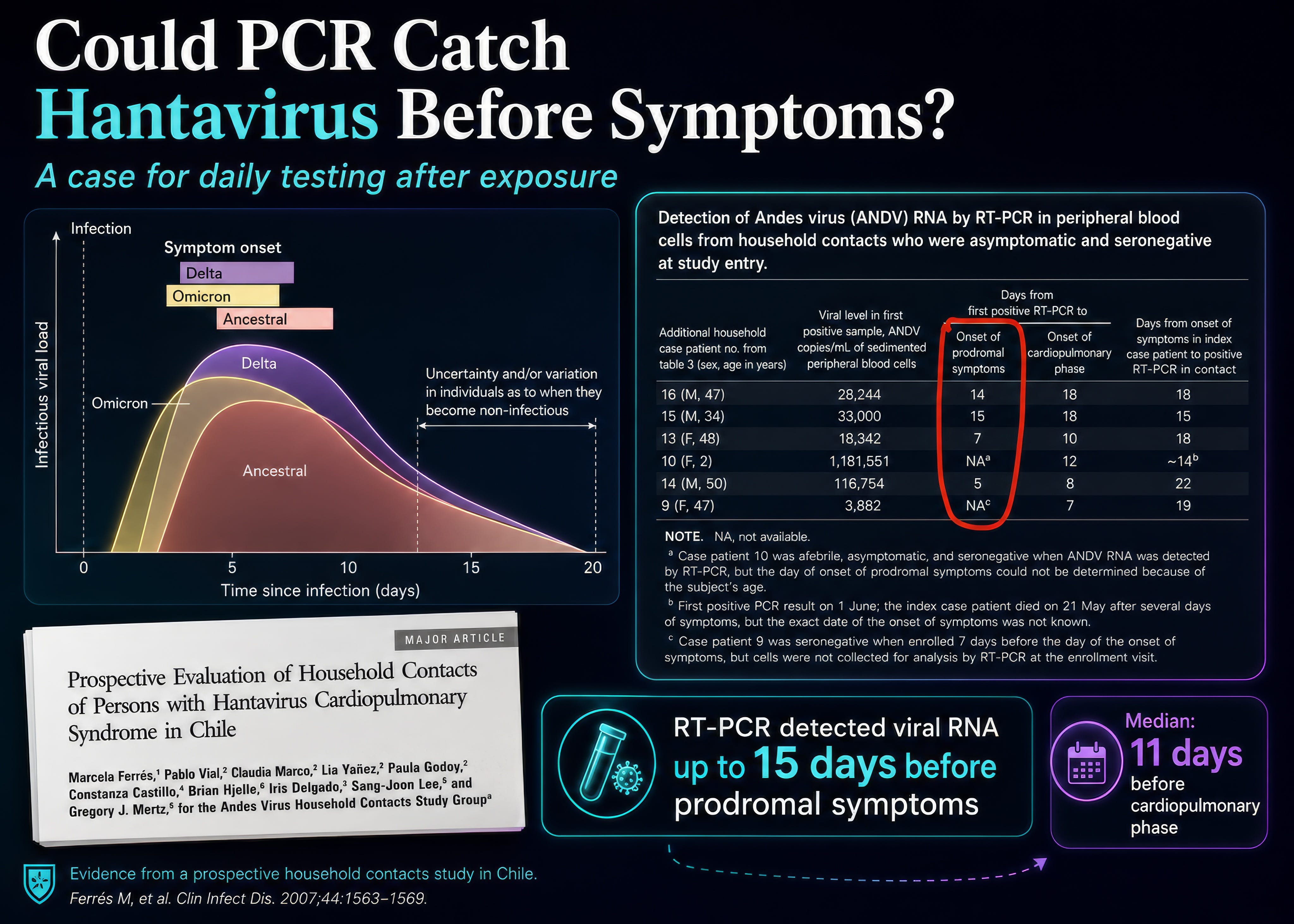
A 2007 study showed PCR tests can detect Andes infection up to 14 days before symptoms. Why isn't this part of "Monitoring"?

I’ve been poring through all the research on hantaviruses, especially this Andes virus (ANDV) from the cruise ship– the only type of hantavirus with demonstrated human-to-human transmission–and I can’t figure out a good answer to this question:
Why are we not conducting daily PCR testing on potential cases to catch and quarantine them BEFORE they become infectious?
When I started researching this, it didn’t seem like any authorities were doing daily testing, but I recently discovered that this is, in fact, the UK policy:
Right now the biggest worry is “What if it spreads from the people who were exposed, and are now being monitored but not quarantined, given the long incubation period?”
There are 32 people who disembarked in St Helena, and then many more who were on a flight to Johannesburg on April 25th with the actively sick passenger who sadly died the next day. In the US, 12 of these people are “being monitored,” but I haven’t seen mention of quarantine or testing.
I was able to find the CDC guidance document for what “monitoring” means, and it reads:
A CLIA Andes virus–specific rRT-PCR assay is not currently available in the United States; once available, it could be used to test symptomatic patients. However, sensitivity may be reduced for specimens collected later in the course of illness, as viremia may be low or undetectable beyond approximately 7–10 days after symptom onset. Detailed guidance for laboratory testing of contacts will be provided separately.”
Why are they not available? This seems like something that it would be very possible for the administration to procure… and administer.
Why Testing Matters
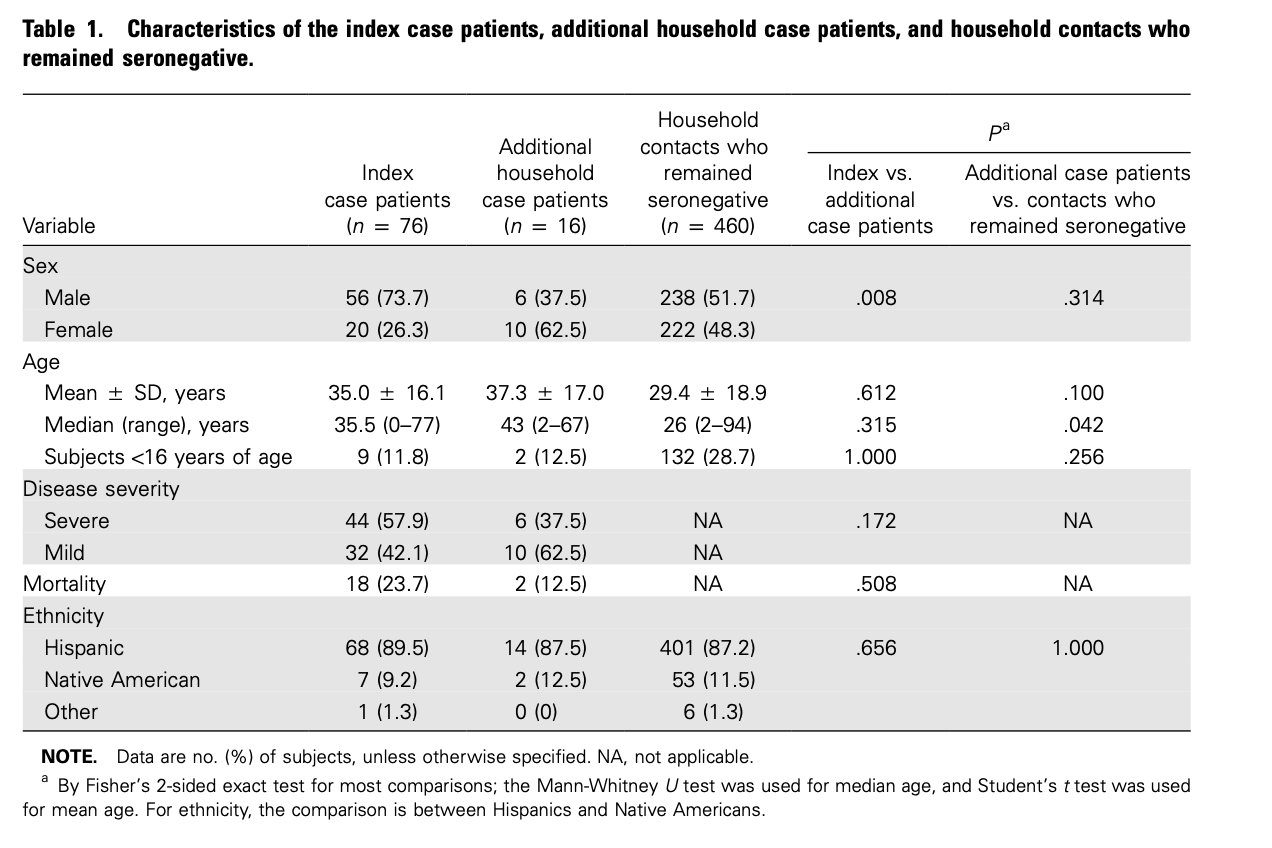
We have very limited data on ANDV and the specifics of how it spreads, and everyone seems to be focusing on the 2018 outbreak and whether that showed airborne spread–which i can cover in detail if you want–but there was another really important study published in 2007. It looked at 76 households with confirmed cases of hantavirus cardiopulmonary syndrome (HPS) between 2001 and 2005. Not an outbreak, just individual index cases most likely from the usual rodent route. But the researchers wanted to see how it spread in those households.
They looked at the 476 household contacts, monitoring them for symptoms and taking weekly blood tests. They analyzed this blood for anti-hantavirus antibodies and performed PCR tests to look for any actual viral RNA. If you remember from COVID, PCR tests can detect very small amounts of genetic material, so they can be positive BEFORE symptoms show and for a while after they go away.
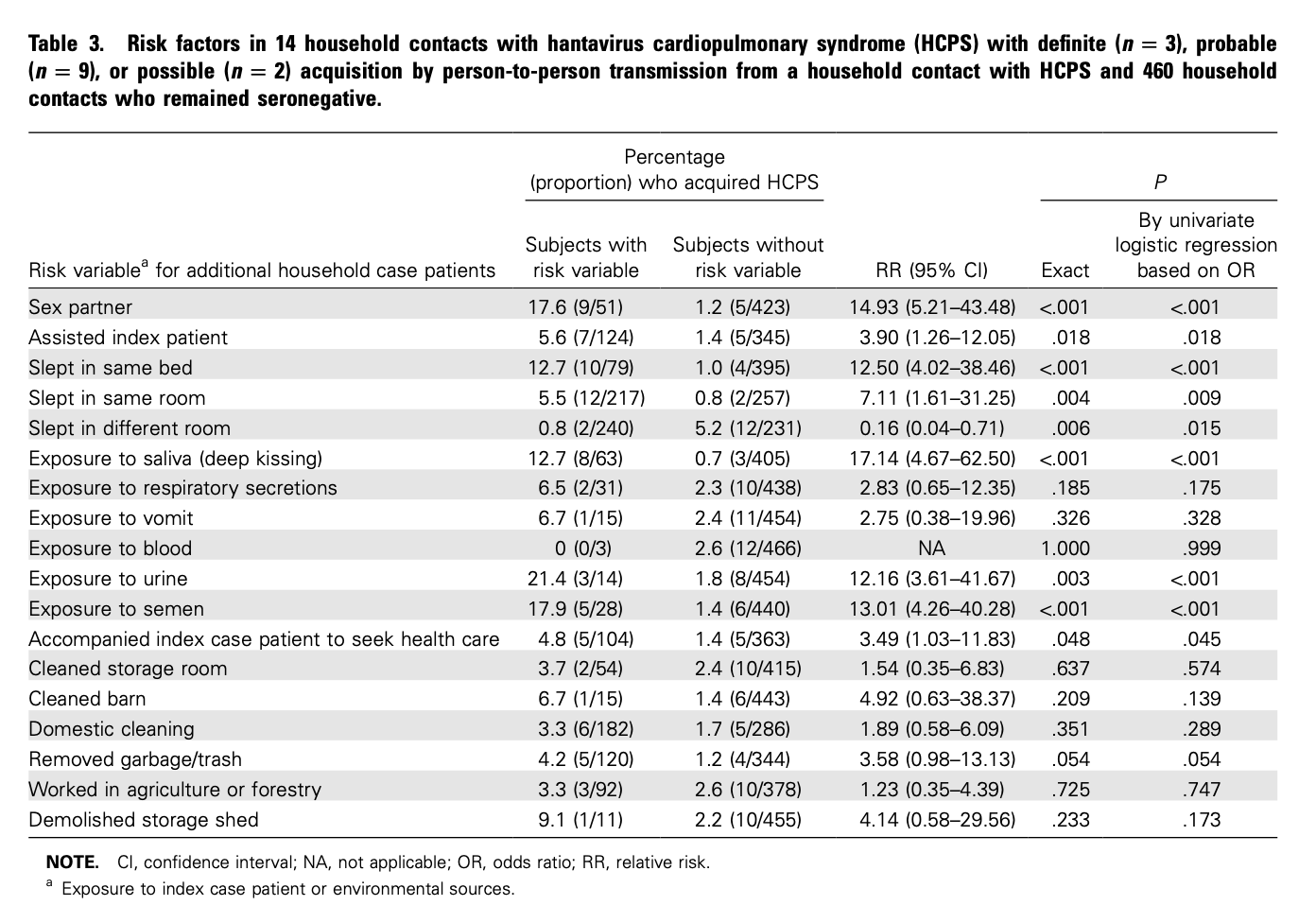
16 household contacts ended up getting sick. Comparing these 16 to the other 460, they found that the risk of transmission was “17.6% among sex partners” vs “1.2% among non-sex partners” - which strongly supports transmission via bodily fluids rather than airborne, but these dynamics seem very different from the 2018 outbreak, and it was a different ANDV strain.

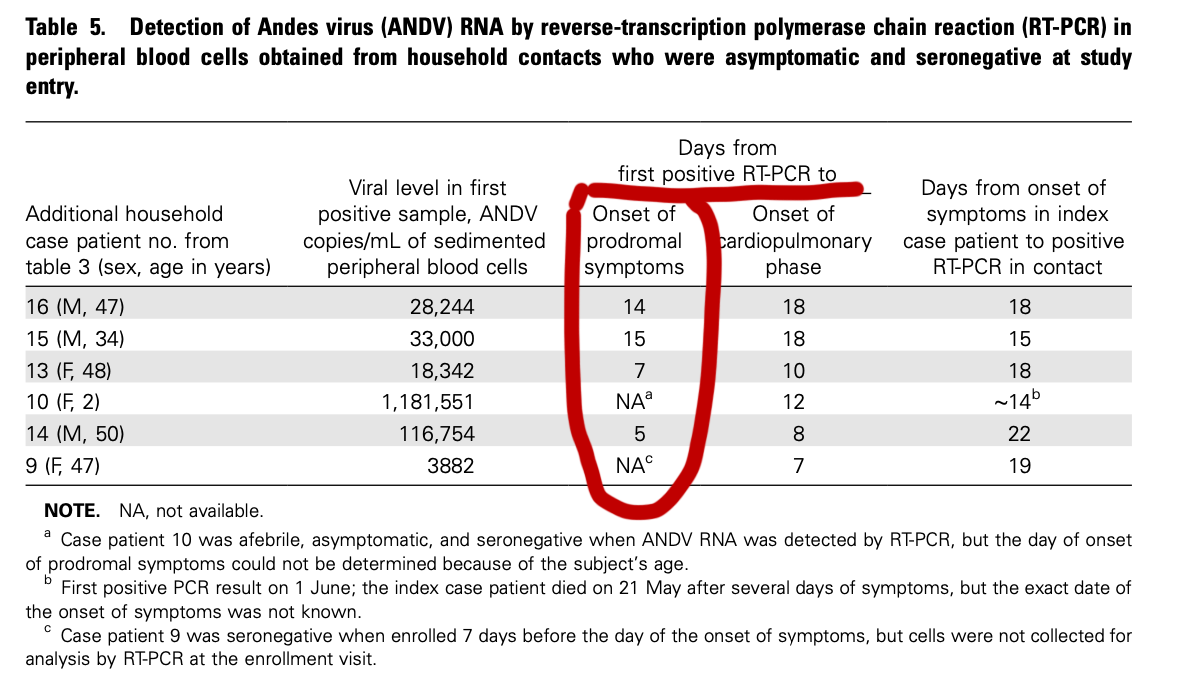
But here’s the key part. They detected ANDV RNA a median of 11 days before the cardiopulmonary phase in 6 household cases, and 5, 7, 14, and 15 days before the onset of the early mild symptoms in 4 additional cases.
Asymptomatic / Presymptomatic Transmission
Right now, we still don’t know whether presymptomatic transmission is possible or likely for ANDV, but we DO know that it is extremely common for most other viruses, even if the peak transmission period is after symptoms emerge.
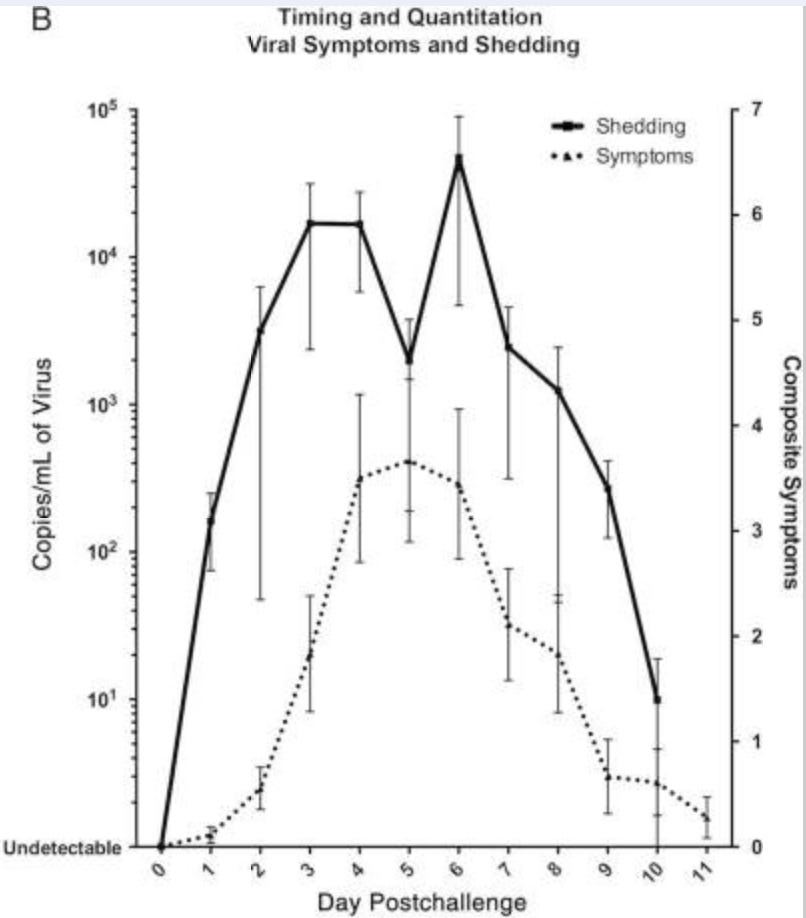
This Influenza human challenge trial showed infected volunteers began shedding virus 24-48 hours before symptoms showed.
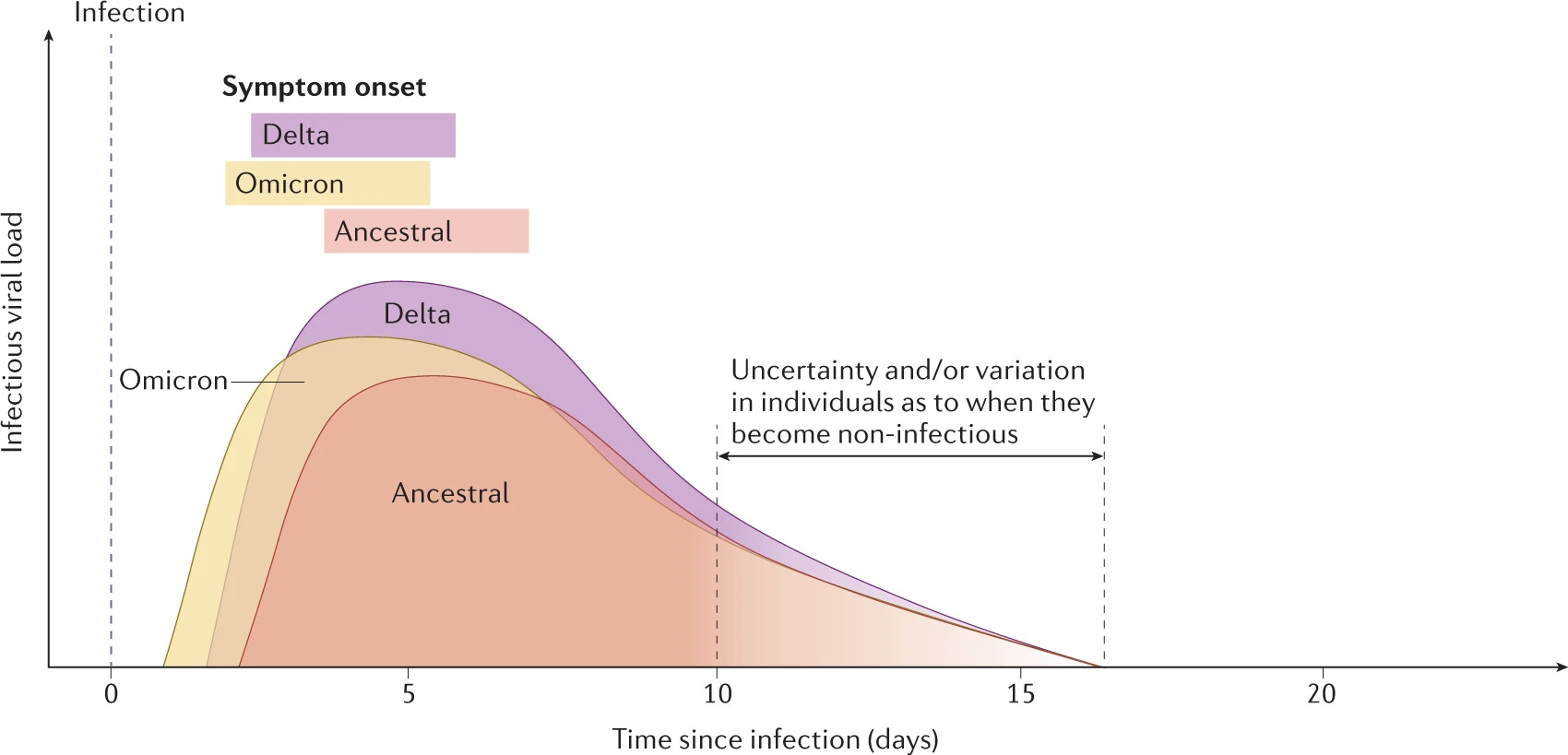
This 2023 Nature review of all the primary COVID variants painted a similar picture: viral load rises rapidly after infection, and it is possible for them to be infectious before symptom onset.
And yet…
Right now, the WHO says that
infectiousness peaks in the early phase of illness, and that pre-symptomatic transmission cannot be entirely ruled out
Which is technically accurate, but it implies that it will be entirely ruled out in the future, rather than the more likely scenario of “some amount of pre-symptomatic infectivity is likely to be possible.”
Similarly, the CDC says that:
Typically, people are only infectious while they have symptoms.
Typically? Sure. But we don’t have enough data yet to know for sure, and now is when it pays to have an abundance of caution.
Conclusion
I get that testing isn’t fun, and comes with its own set of logistical difficulties and added stress for the people getting tested. I feel for them, and I hope that they’re able to go through this with as little stress as possible. But if I had potentially been exposed, I would be lining up to get tested!
The current WHO guidelines read:
Current evidence does not support routine laboratory testing of contacts for outbreak control (or public health response) or the quarantine of low-risk contacts; low-risk contacts should undertake passive self-monitoring and seek medical evaluation if symptoms occur. Recommendations are dynamic and will be adapted as more evidence emerges.”
This makes sense for a large-scale pandemic, where the resources and costs involved in testing every exposed person would be prohibitive. But right now, we are in a critical stage where the number of exposures is small enough that full testing and quarantining are absolutely possible!
I still believe that there is a very low likelihood of this outbreak getting out of control, but I would also like to believe that our public health authorities are doing everything in their power to ensure that that is the outcome.
Why aren’t we testing?